Teaching Points
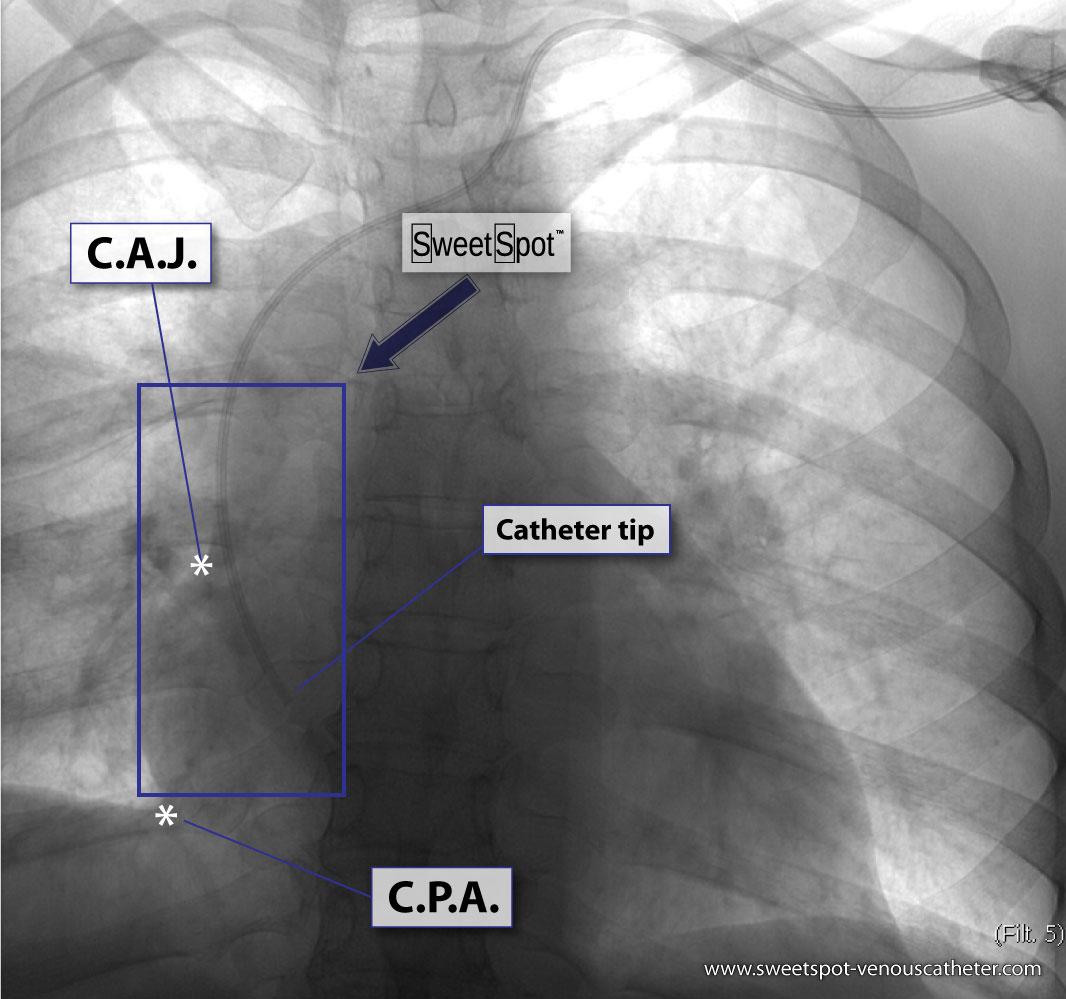
- When I place a VAD under flouroscopic visualization, my optimal tip position is in the bottom of the box at expiration. See Fig.# 25 - Gallery.
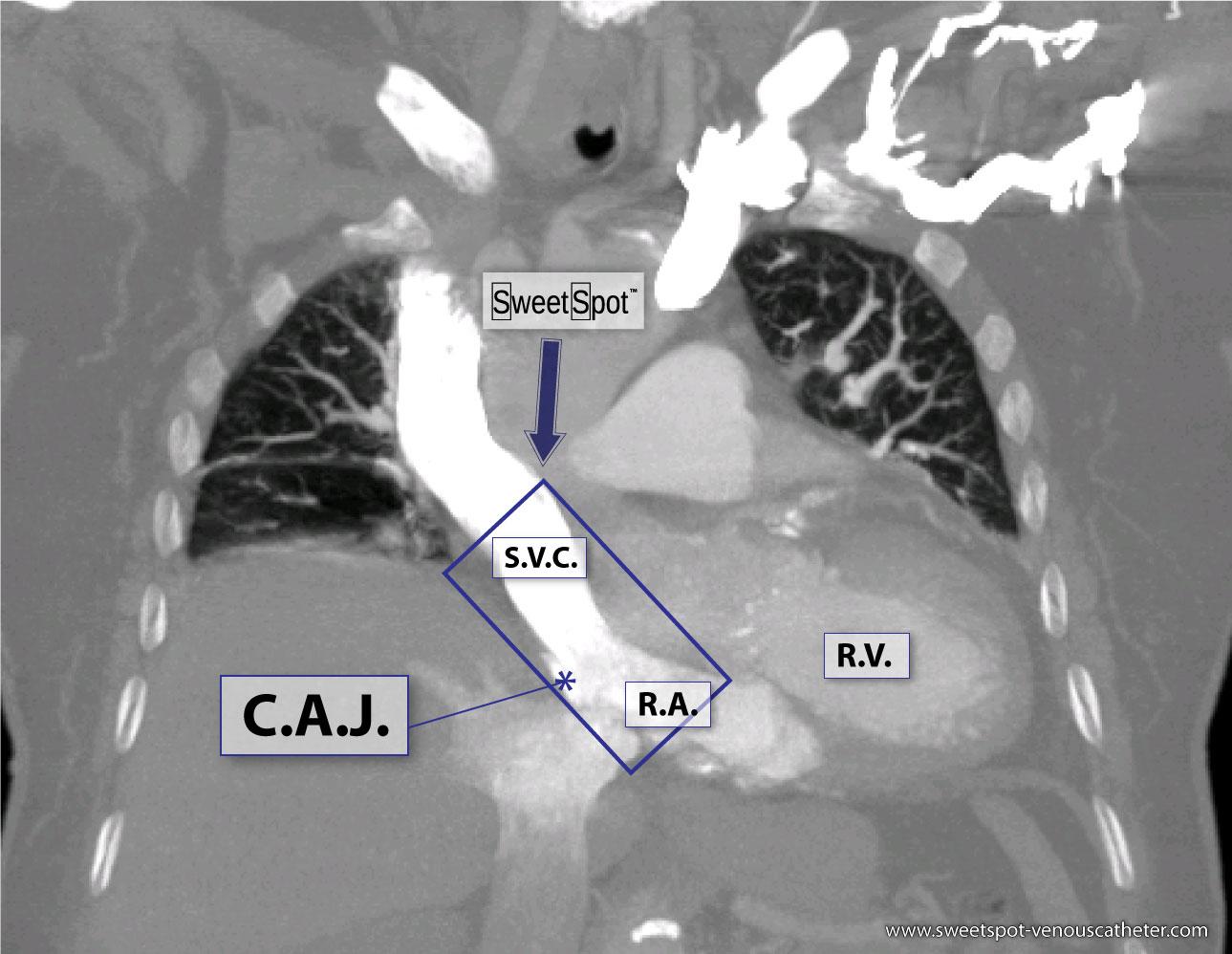
- On inspiration upright CXR, the tip of VAD is ideally at C.A.J. See Fig.# 09 - Gallery.
- Chest x-ray rotation tissues: Not infrequently, the chest x-ray will be rotated causing the right cardiac margin to deviate from its normal AP appearance. In such situations, depending on the degree of rotation, an estimation of the SWEET SPOT™ is all that may be possible. In such circumstances, the right cardiophrenic angle is the most reliable anatomic landmark. Since the right atrium is immediately cephalad to a normally positioned right cardiophrenic angle, a reliable estimation of acceptable catheter tip location is still possible. The height, and consequently the width of the rectangular Sweet Spot™ box will be less exact and therefore a relatively short catheter tip position may require a non- rotated chest x-ray to confirm an acceptable location. Aim for the right atrium. See Figs. T.1, T.2, and T.3.
- Abnormal appearance of the right cardiac border on non- rotated chest x-ray: Again, the cardiophrenic angle is the most reliable landmark and thus the same principles apply as in teaching point #3. See Fig.# 26 - Gallery.
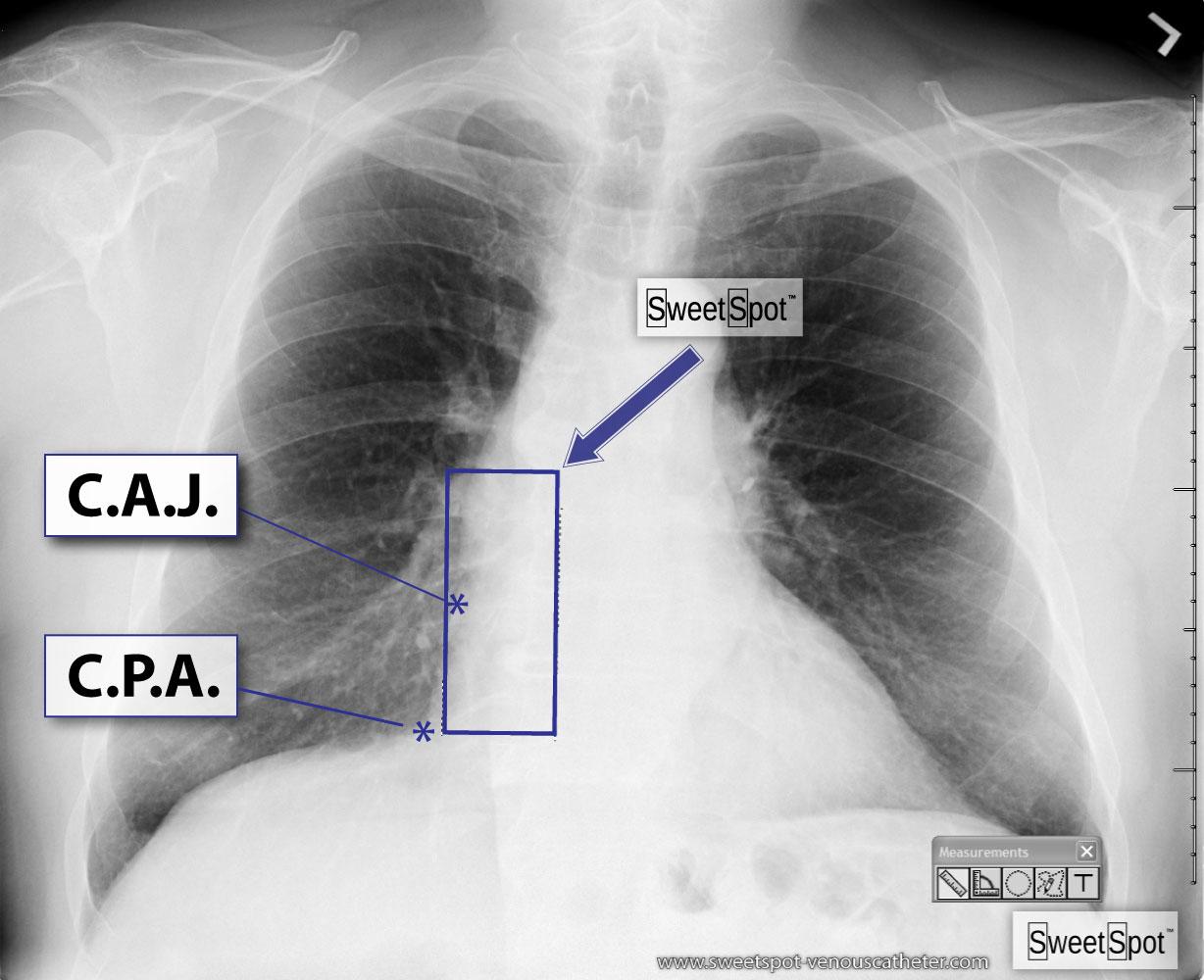
- Assessment of normal position of right cardiophrenic angle: The best way to confirm a normally positioned right cardiophrenic angle is to look at the left cardiophrenic angle. Generally speaking, the right cardiophrenic angle should be at approximately the same height as the left cardiophrenic angle. In the case of an elevated right cardiophrenic angle, experience and a solid understanding of SWEET SPOT™ anatomy may suffice. However with very low lung volumes and bilaterally raised hemi-diaphrams, even this may not be sufficient. See Fig. # 8.
- A left-sided approach often causes the tip of the venous access device to curve to the patient's left, necessitating a relatively wide SWEET SPOT™ design. See Fig.# 10 - Gallery.
- Even on normal frontal chest x-rays, there can be significant variation in the appearance of the cardiomediastinal silhouette which can result in slight subjectivity in the exact location of the margins of the SWEET SPOT™. The closer the catheter tip is to the cavoatrial junction, the less this matters.
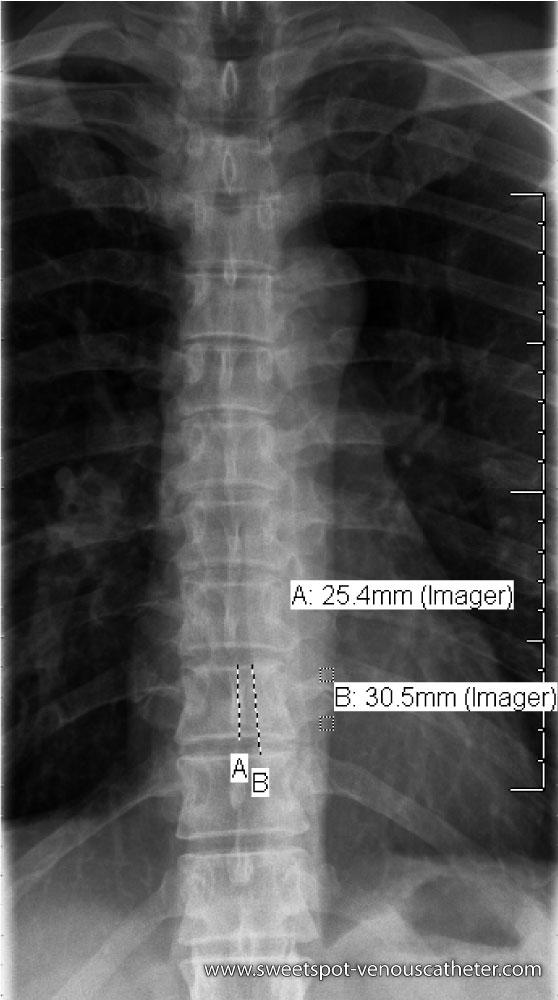
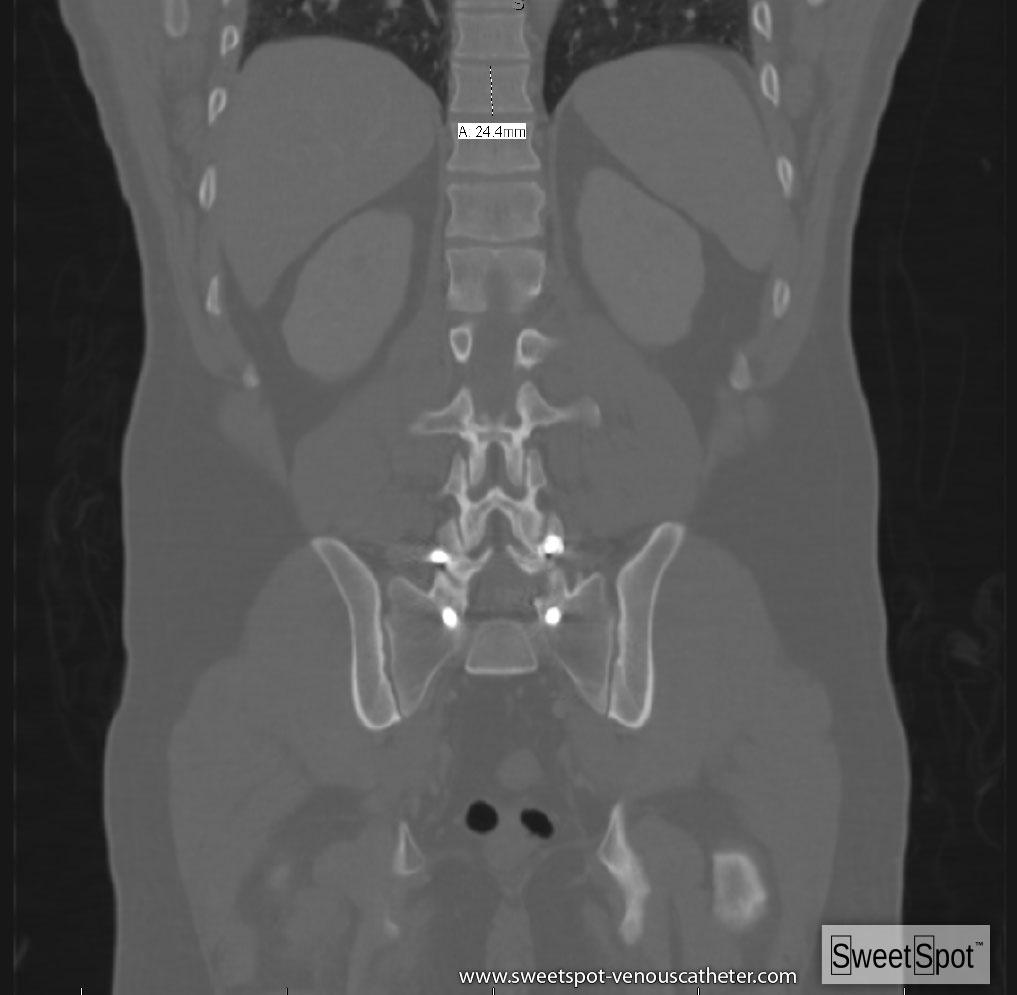
- The height of a normal adult lower thoracic vertebral body is generally about 2.5 cm. This is a very good internal ruler. See Figs. #13 and #14 - Gallery.
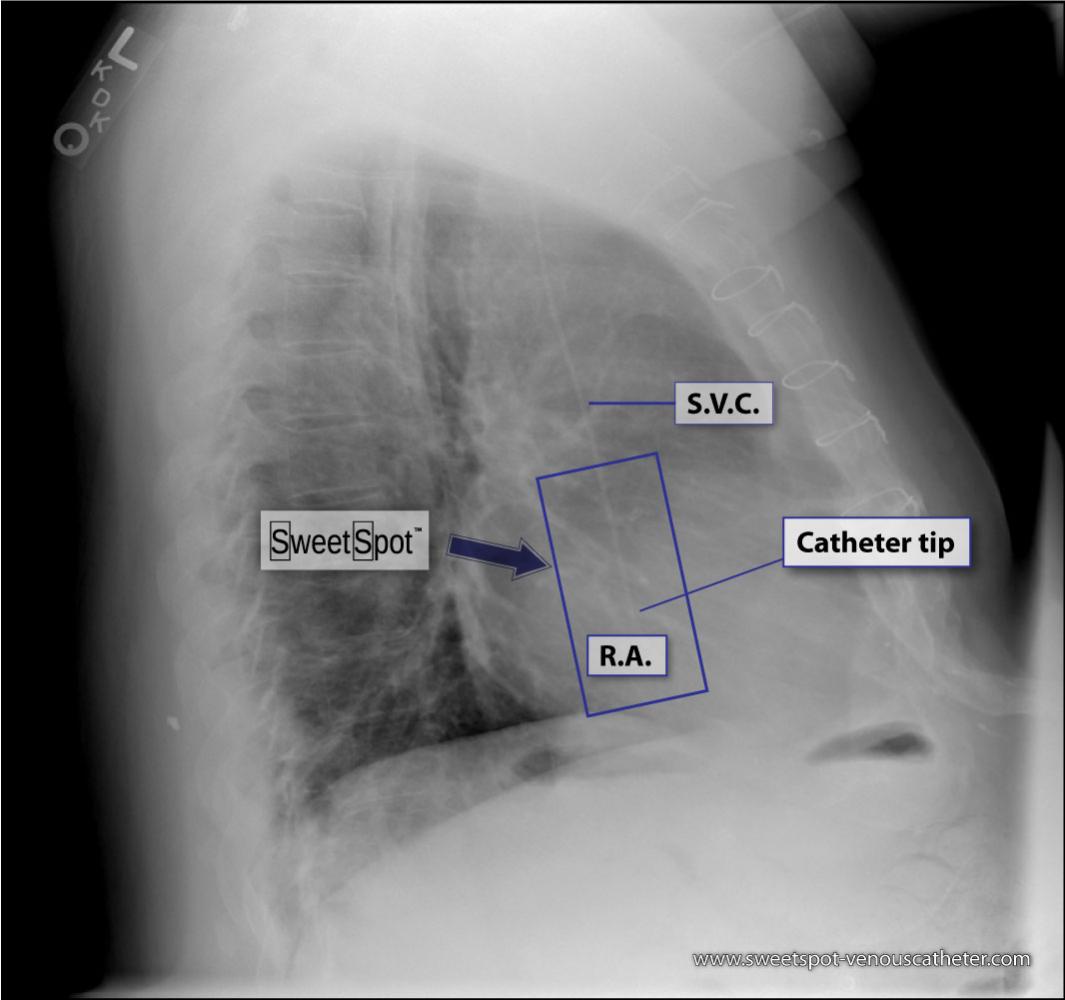
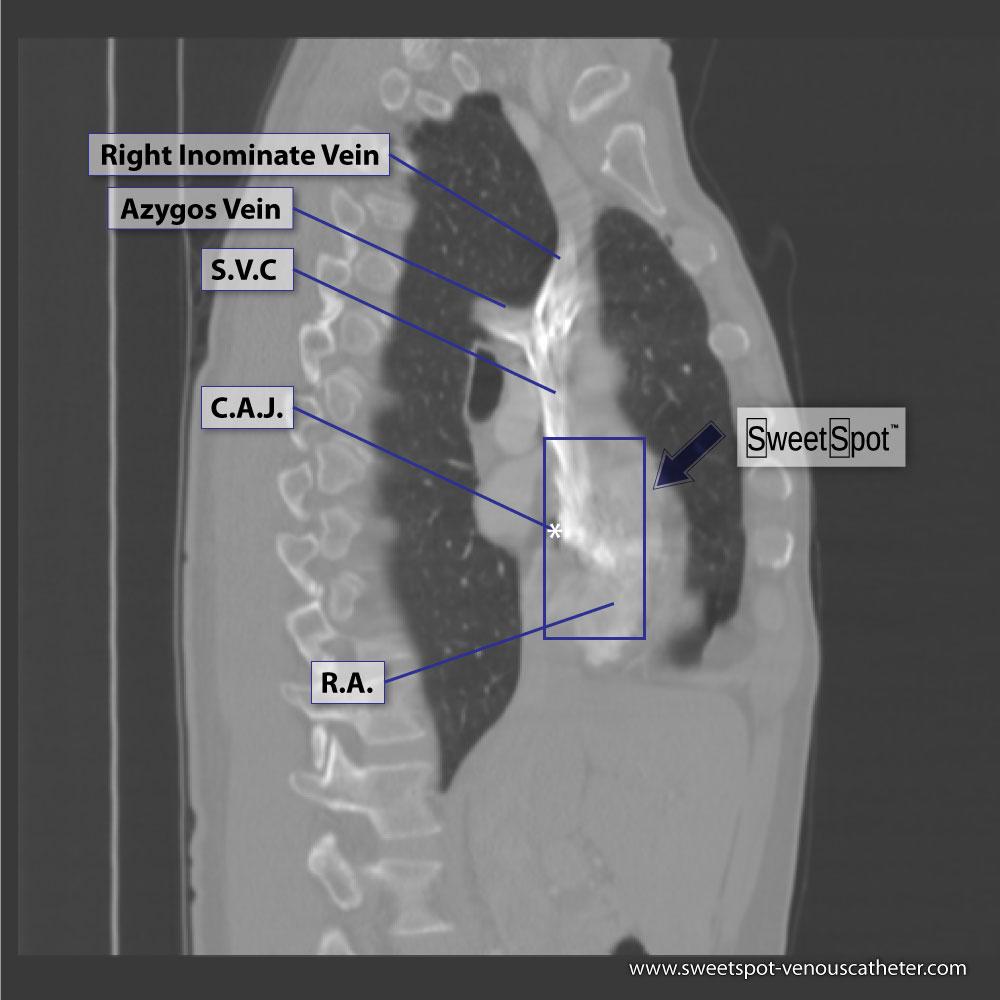
- On a lateral chest x-ray, the catheter should course in an almost straight line from the superior vena cava into the right atrium. If it deviates posteriorly from this straight orientation, suspect that it has entered the azygos vein. See. Figs. #15 and #16 - Gallery. If this is the case, reposition the catheter.
- The superior vena cava is surprisingly long - particularly in patients with a long cardiomediastinal silhouette.
- A catheter tip that is short of the SWEET SPOT™ runs the risk of flipping into the left innominate vein or the right innominate vein( depending on what side access was from) during either the cardiac and/ or the respiratory cycle- causing potential intimal injury / fibrin sleeve / thrombus, etc.. See. Fig. #6 - Gallery.
- If the the patient has low lung volumes and therefore both cardiophrenic angles are in a relatively cephalad location, the patient will correspondingly have a shorter SWEET SPOT™ and a resultant narrower width as well. See Fig.# 19 - Gallery.
- The longer the cardiomediastinal silhouette is the larger the SWEET SPOT™ will be. See Fig.# 19 - Gallery.
- The right margin of the high density cardiomediastinal silhouette is normally seen when low density aerated right lung is adjacent to it. Any process of soft tissue density that is situated at that margin will obscure that margin – proportional to its size. Common examples are pneumonia, atelectasis, tumor & pleural effusion. See Fig.# 26 - Gallery. Also see slide #46 of AVA Presentation.
- If you find that you are having information overload, just try to memorize Fig. #1. (And pray that you do not have CXR Fig.# 28 - Gallery.)
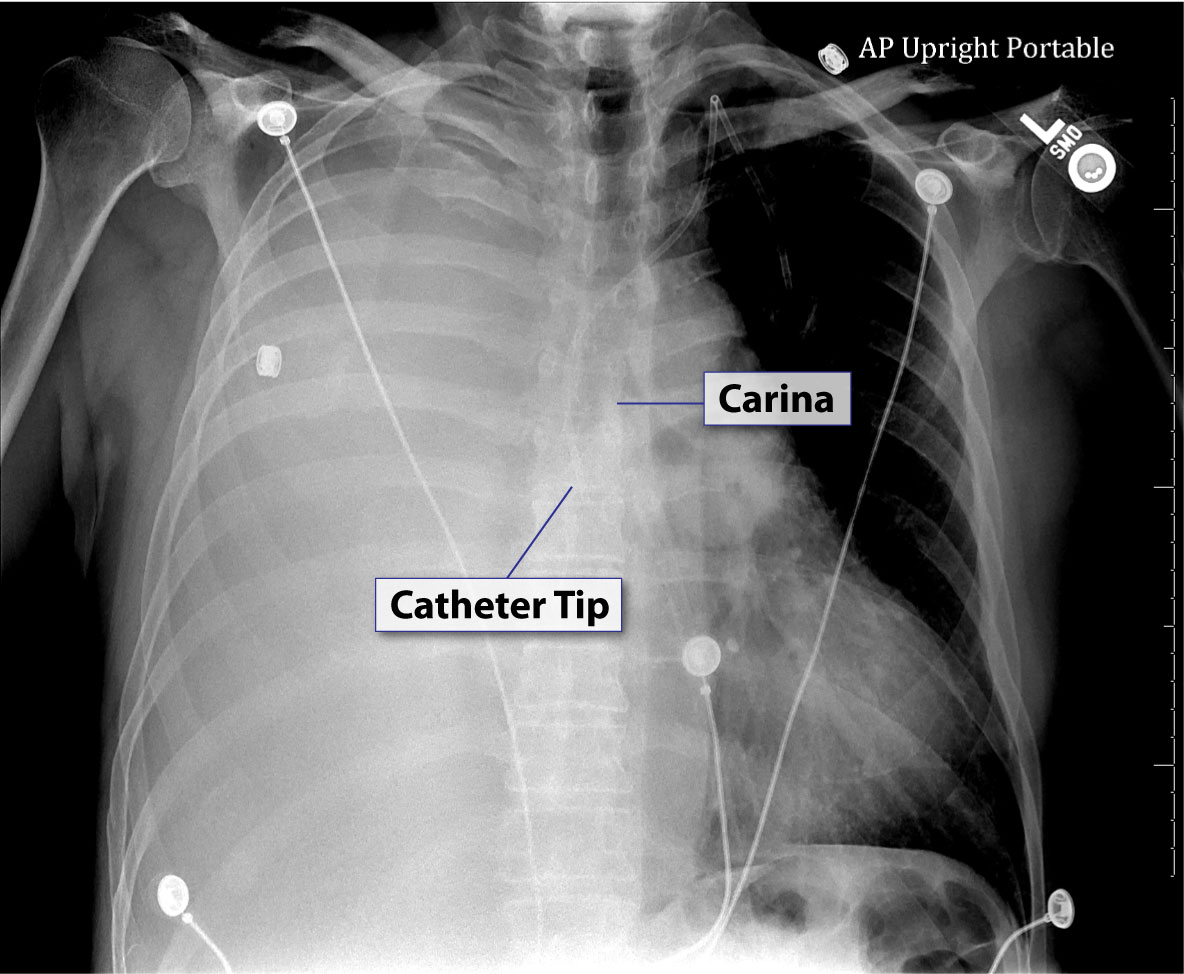
- “A good use of carinal landmarks for catheter tip location- right sided White Out.” See Fig. T.4 - Carina.
Click to thumbnail images to enlarge

CXR Sweet Spot™ Box

CXR Sweet Spot™ Box

CXR Sweet Spot™ Box
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}